

It is not affiliated with Swiss Chems or with any company named here, and it links to no one’s order page. The only outbound links go to primary sources anyone can open directly: the documented FDA actions and the human trials behind these compounds. Compounded or prescribed peptides discussed here are not FDA-approved, and “research use only” products are not approved for human use at all. Last updated June 2026.
Ask someone who is hovering over a Swiss Chems alternative what they actually want to know, and it is almost never “is this legit” or “is this cheap.” It is something closer to biology: if I take this, how does my body decide how much is too much, and who is watching that curve besides me?
That question turns out to have a real answer, and the answer is mostly about a concept most dosing conversations skip past entirely: the dose-response relationship. A molecule does not have one correct dose sitting on a label somewhere, waiting to be copied. It has a curve, low doses doing little, a middle range where effect and side effects both climb, and a ceiling past which more drug just means more risk without more benefit. Finding the useful part of that curve, for a specific person, is what titration means. It is not a bureaucratic word. It is the actual mechanism by which a clinician tunes a molecule to a body.


A week spent chasing that question through the research-chemical corner of this category, and then through the supervised side, turned up a clean split: one side has never built a mechanism for finding that curve, and the other side’s entire structure exists to find it.
The research-chemical side has no titration mechanism, only a number copied from somewhere
Start with the retail and forum layer, where Swiss Chems sits as a fair example, a real, operating seller of peptides, SARMs, and related compounds labeled “for research use only” and “not for human consumption.” It is more upfront than a lot of competitors. It publishes certificates of analysis on parts of its catalog, and in its own terms it does not hand out dosing guidance or pretend to condone personal use. That is honest, as far as it goes.
But it also removes the one thing dosing actually requires: a feedback loop between a specific body and a specific dose, observed over time by someone qualified to read the result. Without that loop, the “dosing” people quote in forums and Telegram groups is not titration at all. It is a borrowed number, stated with a confidence that has nothing behind it. Nobody in that chain knows whether the vial in a given hand matches its label at the stated strength, and a certificate of analysis does not fix that gap. A certificate verifies a tested sample. It says nothing about the vial that actually ships, and nothing about whether that dose sits anywhere near the useful part of a given person’s curve. What looks like protocol is improvisation wearing a lab coat.
Regulators have been describing the same gap, from the outside
While tracing this, the 2026 enforcement record kept surfacing, because the legal ground under the whole model has been moving.
On April 7, 2026, the FDA posted warning letters, dated March 31, to online peptide sellers including Gram Peptides and Prime Sciences, calling the products unapproved new drugs and rejecting the “research use only” label outright. The agency’s own language: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C1]. That followed a documented wave of more than fifty warning letters in a single September 2025 stretch, targeting compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use” [C2].
To be fair, no FDA letter to Swiss Chems specifically turned up in this reporting, and none is implied. The named sellers are other companies. What matters for the mechanism question is structural, not personal: the self-source, self-dose, “research label” model is exactly the pattern the agency spent a year dismantling [C1][C2]. A curve nobody is tracking is risky biology. It is also, increasingly, standing on ground the FDA has been actively pulling out from under it.
What the trials actually show about titration, mechanism first
Here is where the biology gets genuinely interesting, because the two best-known GLP-1 molecules are a useful lesson in how a dose-response curve gets managed properly.
Semaglutide and tirzepatide both work by mimicking gut hormones (GLP-1, and in tirzepatide’s case, GIP as well) that signal fullness to the brain and slow gastric emptying. That mechanism has a real curve: too little and nothing much happens, too much too fast and gastrointestinal side effects spike before any added benefit shows up. So the actual clinical protocol for these drugs is a slow dose escalation, weeks at each step, with the clinician watching tolerance before moving up. That is not a bureaucratic add-on to the drug. It is how the drug’s own biology has to be managed.
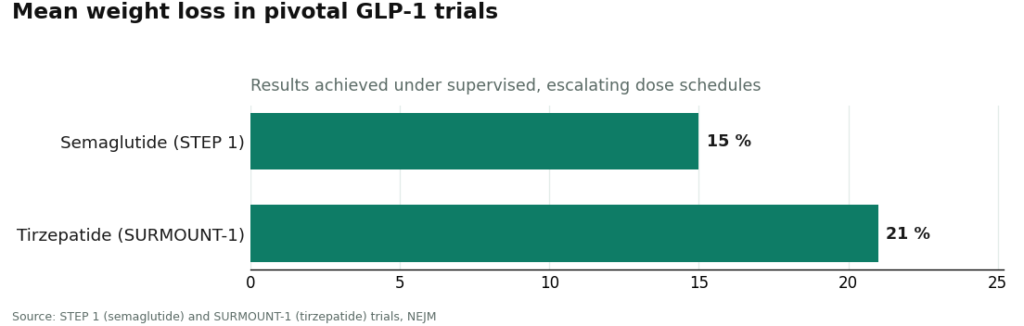
The trial results reflect exactly that supervised process. In STEP 1, semaglutide produced about 15 percent mean weight loss [C3]. In SURMOUNT-1, tirzepatide produced about 21 percent [C4]. Those numbers came out of careful, monitored dose escalation, not out of someone estimating a starting dose off a forum thread and adjusting by feel. The titration was part of the mechanism that produced the result, not a footnote to it.
Where the trials and the real world diverge
This is the gap worth sitting with. The impressive numbers above describe what happens when a clinician owns the curve. They do not describe what happens when a research-chemical buyer owns it instead.
A supervised pathway is built to reproduce the trial conditions as closely as a clinic can: a licensed clinician reviews history and medications, decides whether a compound is appropriate at all, sets a starting dose, and adjusts it based on how the person actually responds. As one entity operating this kind of supervised access in 2026, FormBlends routes people through independent licensed clinicians with a required prescription and dispenses through licensed 503A compounding pharmacies, named here as an illustration of that structure rather than a product to shop for. The medicine itself gets verified per batch by a pharmacy with a license to lose, which is a different claim than a certificate verifying one tested sample somewhere upstream. And the honest ones say plainly, in the wake of the 2026 letters, that compounded medicine is not FDA-approved and not reviewed for safety or effectiveness the way an approved drug is [C2]. A provider willing to be straight about that status tends to be straighter about a realistic dose, too.
None of that closes the gap for every molecule, though, and pretending otherwise would be its own kind of overselling. BPC-157, one of the most-searched peptides in this space, has an interesting proposed mechanism as a cytoprotective agent, but the evidence behind it is still overwhelmingly preclinical, mostly animal models, according to a 2026 review in Pharmaceuticals [C5]. Perfect titration under perfect supervision still would not turn that evidence base into human proof. Titration manages safety and dose. It does not manufacture efficacy that the trials have not shown yet.
SARMs sit outside this entirely. They are not approved for human use, the FDA has flagged serious safety risks, and no legitimate clinical provider offers a supervised dosing pathway for them. There is no titration mechanism to describe, because the clinical structure that would run it does not exist for these compounds.
A small tool that actually helps close the loop
One unglamorous detail from the supervised side is worth mentioning because it directly serves the titration mechanism rather than just sounding responsible. A dose, a date, and a note on how someone felt, logged consistently (people using the FormBlends tracker app do this, for instance) turns a vague memory into data a clinician can actually titrate against at the next check-in. It is a logging tool, nothing more, not a prescription and not a checkout. But it is the kind of record that lets a clinician see the shape of an individual’s curve instead of guessing at it. The research-chemical model has no equivalent, because there is no clinician on the other end reading it anyway.
The takeaway
Choosing here is really a choice about who manages the dose-response curve. In the research-chemical world, that job falls to the buyer and a forum, with a certificate that verifies a sample rather than the actual vial or the actual person taking it. In a supervised pathway, a licensed clinician screens, sets, and adjusts the dose, a licensed pharmacy verifies the medicine batch by batch, the provider is upfront that compounded is not FDA-approved, and someone stays reachable after the first order. That is the structure the 2026 enforcement wave has been quietly pushing the category toward [C1][C2]. What it buys is accountability and a properly managed dose. It does not buy FDA approval, and it does not turn a thin-evidence peptide into a proven one.
The questions that keep coming up
How do I figure out the right dose for a research peptide?
From a research-chemical vendor, there is no real mechanism for this, which is the core finding here. Sellers, including ones as transparent as Swiss Chems, do not provide dosing guidance, so numbers circulate through forums and self-styled “coaches” with no way to verify a specific vial or a specific person’s response. Finding a safe, useful dose requires a titration process, a clinician setting a starting point and adjusting based on observed response, which only exists in a supervised pathway.
What does “real oversight” actually mean, mechanically?
Five concrete pieces: a licensed clinician decides whether the compound is appropriate at all, that clinician sets and adjusts the dose through titration rather than a fixed guess, a licensed compounding pharmacy verifies the medicine per batch rather than relying on one posted sample, the provider states plainly that compounded medicines are not FDA-approved, and there is follow-up contact after the first order to keep tuning the dose. A model that ends at checkout has none of these built in.
Is a posted certificate of analysis the same as a managed dose?
No. A certificate verifies a tested sample, not the specific vial that ships, and it says nothing about where a given person sits on that molecule’s dose-response curve. That is genuinely more transparency than vendors offering nothing at all, credit due to Swiss Chems there, but it is not a substitute for per-batch pharmacy verification tied to a prescription and a clinician actively titrating the dose [C1][C2].
Does proper titration mean the peptide will work?
No. Titration manages safety and dose, not proof of efficacy. The GLP-1 molecules have strong trial evidence behind their mechanism and their results, about 15 percent mean weight loss for semaglutide in STEP 1 and about 21 percent for tirzepatide in SURMOUNT-1 [C3][C4]. A compound like BPC-157 has an interesting proposed mechanism but rests mostly on animal-model evidence so far [C5]. Good dosing makes a process safer and accountable. It does not fast-forward a molecule’s evidence base.
Where should someone actually buy from instead of Swiss Chems?
It depends on the goal. For legitimate clinical use, a physician-supervised compounding pharmacy, such as FormBlends, is the accountable path, because a licensed prescriber reviews the case and the pharmacy answers to state boards. For credentialed researchers, an institution’s procurement office exists for exactly this purpose. Skipping both routes trades accountability for convenience, and that trade rarely pays off.
Is Swiss Chems legit, or operating in a gray area?
Swiss Chems sells peptides and SARMs labeled “for research only,” which places it squarely in the regulatory gray zone most research-chemical vendors occupy. That label does not make a vendor a scam, but it does not make it a regulated pharmaceutical supplier either. No U.S. federal agency has certified its products as safe or accurately dosed for human use, and third-party certificates of analysis vary widely in who performed them and what exactly they tested.
What makes a Swiss Chems alternative genuinely better rather than just better marketed?
A genuinely better option has a traceable accountability chain, someone with a license to lose standing behind both the product and the dosing decisions. That typically looks like a state-licensed compounding pharmacy, or a research supplier tied to institutional procurement with independently verified testing. Language like “pharmaceutical grade” or “highest purity,” without a named accredited lab and a clear chain of custody, is not evidence of anything.
Can online reviews of Swiss Chems be trusted when deciding where to buy?
Treat them as one data point, not a verdict. Reviews say something about shipping speed and customer service, but nothing about whether a compound was accurately dosed or free of contaminants, since most buyers have no independent way to test that. A vendor can carry thousands of positive reviews and still ship product that drifts from its label. Reviews and rigorous quality verification measure entirely different things.
References
- [C1] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the FDA warning letters posted April 7, 2026 and dated March 31, 2026 to sellers including Gram Peptides and Prime Sciences, including the FDA statement that despite “Research Use Only” labeling, website evidence established the products were intended as drugs for human use.
- [C2] Health Law Alliance (Martha Rumore, Esq.), “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling” (January 2026). Documents the September 2025 wave of 50-plus FDA warning letters over compounded GLP-1 marketing and peptides sold “research use only” where advertising indicated human-use intent, and the position that.
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C5] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Gabriel Jain, health-data reporter. Cross-checking the claims against the primary sources. Last reviewed June 2026.
This piece is for learning, not prescribing. See a licensed provider before acting on it.



